


Building Healthcare & Leading Change: Slides from October's lectures
Building Healthcare & Leading Change: Slides from October's lectures
How do you literally build the healthcare of the future? And what do you do when you lack resources to help patients like you’ve done in the past?

I. Two different yet similar worlds
I was recently invited to speak at two very different events. Despite being so different, both addressed the questions above, but from different perspectives. The events were:
The Swedish Rheumatology Leadership Summit - where I led a seminar on leadership and technology
The 4th National Smart Hospital Conference - where I held the inaugural keynote
When I say the events were very different I really mean it. This is DALL-E’s visualization of the two overlapping worlds.
When hospital builders and clinical leaders meet. To DALL-E 3’s credit there are several insightful details.1
The events were very different. One was an intimate gathering of the senior leadership of rheumatology in Sweden – clinicians that have met tens of thousands of patients, as well as led and shaped the practice of rheumatology in Sweden. The other was a large conference which gathered healthcare system leaders, politicians, public servants, and architects – people involved in building future hospitals and healthcare systems.
This Venn diagram explains it in another way:

I normally receive requests to share slides or recordings after I’ve held a talk. After these two talks I received an exceptionally large number of requests - and that’s why I decided to share my slides in this post. Here they are:


The slides above are the short answer to what I talked about.
The text below is the longer answer to why I talked about those things.
And at the very end you'll find a bonus: the answer to what we can learn from combining the lessons from these two events.
II. Leadership & Technology
Context: Rheumatology has historically gone through big changes. In 1998 a new type of treatment (biologic agents) was approved by the FDA and started entering clinical practice. These drugs are very efficient but also quite expensive, which presented a challenge to systems that wanted to prescribe them.
There are similar challenges today. There are new (expensive) therapies and digital monitoring systems that can improve patient outcomes, but introducing these with constrained budgets in an aging population requires change - in budgets, culture and in ways of working. However, to quote Boromir: one does not simply change healthcare.

The session: Historically, many improvements in healthcare have been driven by technology, and understanding and implementing new technologies has been central in improving healthcare systems. I believe that leadership and technology will continue being deeply interlinked and therefore led a conversation on that topic. So in my talk I presented some data on historical demographic and technological changes, posed a couple questions which were discussed in small groups, and then we discussed our answers in the larger group.
This slides summarizes the participants’ answers to three of the questions (click to enlarge):

III. The Best Way to Predict the Future
Context: It’s difficult to build a house. It’s really difficult to plan and build a group of physical buildings for a healthcare system 10-30 years from now as we…
Know that healthcare will not work like it does today, and
Have no idea how healthcare will work, and
Are painfully aware of (a) + (b)
Turns out that planning hospitals is tricky
Planning to be flexible may sound good, but is difficult when you’re in charge of a billion dollar project and have to make decisions. So what do you do?
To be honest, I don't know.
But I think reasoning from first principles can help. In other words, if we can find relevant foundational truths, these might help us make slightly better decisions when it comes to planning the future infrastructure for healthcare.
I should warn you, preparing this text took me deep down some weird rabbit holes.2

A. Fundamental trends
Several trends will continue to impact healthcare systems throughout the western world. Some of the more relevant ones are that we will continue:
Getting older: For example, Sweden’s population is forecasted to grow by 20% until 2070. Half of that increase will occur in the 70+ demographic. Other western countries have similar forecasts with equally dramatic increases in the elderly. It seems as though we will continue getting even older in the foreseeable future.
Gaining access to more effective treatments: Healthcare has revolutionized outcomes for many patient groups. One of my favorite examples is an unsung miracle that happened during the past 15 years in Sweden. The number of heart attacks was reduced by ~50%, and heart attacks are now 50% less lethal.

Humanity has developed an impressive global collaboration between academia, industry and clinicians, which despite all its flaws is propelling medicine forward at a breakneck speed. It seems as though we will continue getting more effective treatments in the foreseeable future.
Becoming increasingly specialized: The more knowledge we accumulate, the more we need to specialize in order to apply it. As we accumulate medical knowledge over time, healthcare providers become more and more specialized. In the 1960s ~6500 US physicians entered a internal medicine residency, and ~450 entered a sub-specialty, i.e. a ratio of around 7%. By the 2010s the ratio had increased to 88%. The same trend is clear in other countries as well. It seems as though we will continue to become more specialized.

B. Consequences from these trends
The three trends have many consequences for healthcare systems. I believe three consequences are particularly relevant for constructing hospitals. Namely, that we can expect:
An increasing number of care modalities: 70 years ago a hospital had inpatient wards, operating rooms, and inpatient clinics. Due to better treatments and increased specialization many processes have been standardized, and an increasing number of patients enter increasingly standardized pathways.3 Today, all hospitals have expanded with more functions (intensive care units, intermediary care units, radiology etc.), more specialties and more modalities (home care, virtual care, remote monitoring, hospital-at-home, palliative care etc). 20 years ago hospital-at-home seemed like science fiction to many providers, but today it’s reality. Based on the underlying drivers, it seems highly probable that we will continue to see new modalities, including some that today may seem like science fiction.
Decreasing length of inpatient stays: Between 2000 and 2017 nearly all OECD countries saw a decrease in the average length of stay in hospital. During that time the average length of stay for a heart attack patient decreased from 9.6 to 6.6 days.4
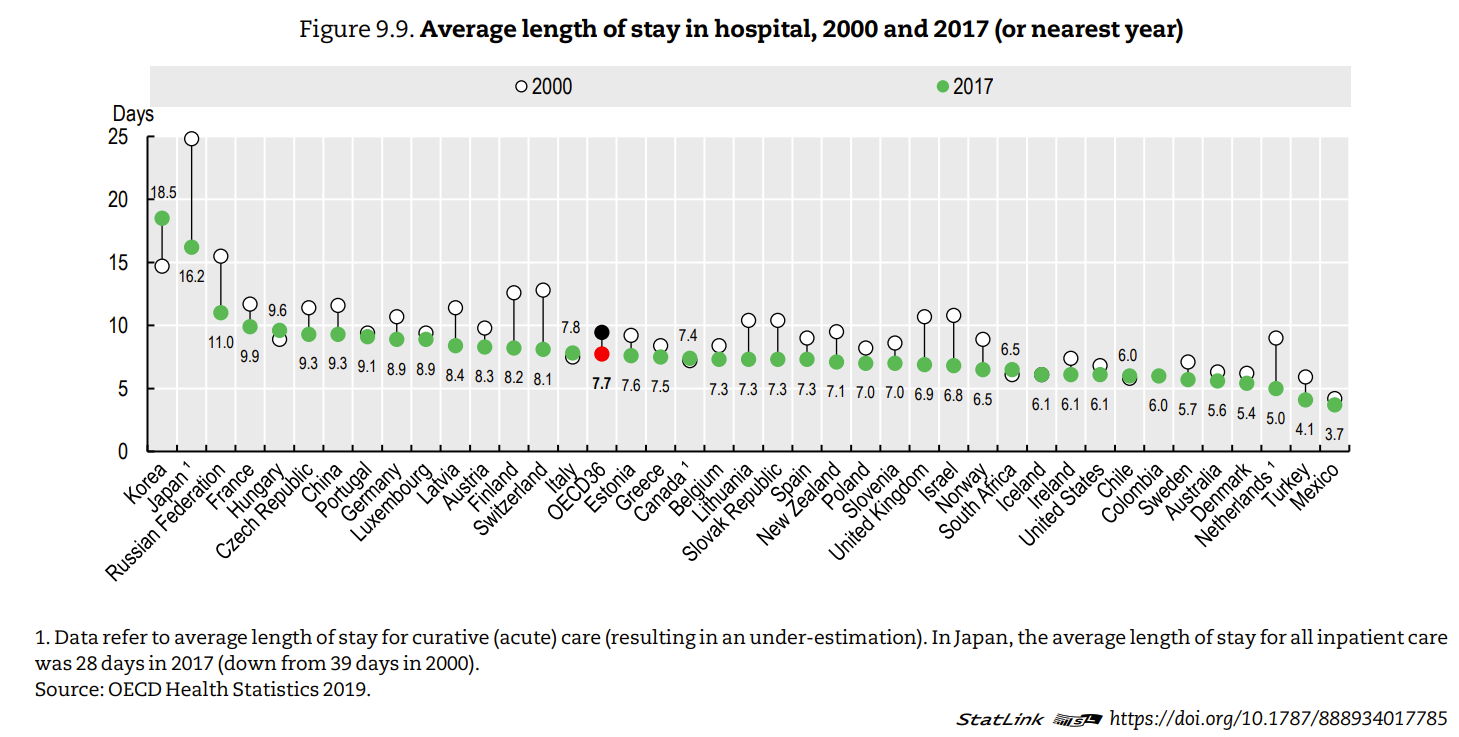
Graph taken from this 2019 OECD report5
If we continue to have more efficient treatments, an older demographic (i.e. a higher need of healthcare), as well as new care modalities allowing care to be delivered efficiently outside of a hospital ward, it’s reasonable to expect that the average length of hospital stay will continue to decrease.
An increasing need to automatically prevent adverse events & complications: I have a friend who's an orthopedic surgeon. A colleague sent him this picture to cheer him up one day when he’d had a tough day operating, saying something like “No matter how bad your day was, you’ll never be as bad as this”.

This is an extreme (but true) example - not only of how bad humor orthopedic surgeons have, but also of how high surgical mortality used to be. In Liston’s era (the 18th century), the amputation mortality rate was ~25%. At that time the main focus for clinicians, patients and providers was to make sure the procedure didn't kill the patient. Healthcare associated injuries and healthcare associated infections (HAI) were neither well understood nor highly prioritized.
However, as treatments improve, the relative importance of these complications increase compared to the patients' underlying treatment. Similarly, the shorter the average in-hospital stay is, the larger the economical and operational impact of HAI. In the 1960s, when an average in-hospital stay for a patient with a heart attack was a month6 - a catheter associated urinary tract infection didn't really create any operational challenges. But the shorter the stay (and the fewer hospital beds providers have), the higher the opportunity cost of those HAI. This relative importance will only continue to increase.
C. Implications for future hospitals
Based on the consequences above, hospitals of the future will need to be designed to handle:
Increased flexibility for novel care modalities: We are seeing many new modalities. We can plan and design for the new ones that will emerge during the coming 30 years. One way is to look at other healthcare systems which have successfully implemented and retained a new modality. A concrete example is Hospital at Home (HaH).
Hospital at home is a care modality where patients who are stable but still need hospital care are discharged to their home earlier than usual. They are monitored by healthcare staff using digital monitoring systems. The staff can either perform virtual consultations, or visit the patient if needed, and examine them or administer treatments.
In the US HaH has grown a lot during the last 20 years, and is now spreading to other European countries. HaH requires healthcare staff to be able to reach patients quickly if they deteriorate. In physical terms, this may require a greater need for parking spaces for staff, or smaller hubs in central areas where staff can store medical equipment and have cubicles for virtual meetings.
There are many examples of other modalities (remote patient monitoring, working from abroad, more interventional radiology, etc) and depending on the hospital's profile, different modalities will be more or less relevant.
Higher patient turnover: A growing and aging population, with increasingly shorter in-hospital stays, will result in a higher patient turnover. This means:
A greater need for more physical space for patients being admitted and discharged: Often times, the ability to discharge a patient is a big bottle neck. Some hospitals have solved that by building patient hotels adjacent to the hospital, whereas others establish partnerships with municipal short term facilities.
An opportunity to scale the effects of more aesthetic rooms.
Pop quiz: which of these two hospital rooms would you prefer to stay in?

I think most people will intuitively be drawn to (B). Having beautiful windows with a view of nature is less important than hard medical outcomes like mortality, injury and pain. However, daylight and views of nature seem to have beneficial effects on relevant outcomes such as less pain, shorter stays, better sleep, better employer satisfaction7. As healthcare treatments improve, these potentially small effects become increasingly important - especially as patient turnover increases.
The higher patient turnover, the greater number of patients can benefit from a more esthetic room. In other words, the marginal cost goes down per patient, and esthetic patient environments gain scale.

More technical and automated preventive technology: It's tempting to believe that we can simply create guidelines to prevent complications like HAI. However, look at the graph below.

A review published in 2010 found 96 studies looking at hygiene compliance rates and found an overall median compliance rate of 40%. Yikes.

We still struggle to change our behavior to improve hygiene and prevent complications. I believe the only way to consistently reduce HAI and other complications at scale is to automate the prevention, i.e through technology.
What do I mean? Well, concrete examples of this include:
Fall detection systems to prevent fall injuries: Many patients fall when at hospital, and that can lead to very serous consequences. Every year fall injuries cost $1.6B in Sweden alone (with a population of 10 million). There are new technologies like radar and camera systems that can intelligently detect patients at risk, and alert healthcare staff when a wobbly patient starts getting out of bed and thus prevent fall injuries. n
Smarter ventilation systems to decrease surgical site infections: in Sweden, surgical site infections kill more patients every year than the total amount killed in traffic accidents. There are many new devices that can reduce the infection rate more than older legacy ventilation systems.
I think we'll see a growing need for preventive systems like those mentioned above - and that it's something one should plan for when building new hospitals.
Thanks dear reader for reading this far! If you’ve read everything until now I think the final summary slide in the handout (hopefully) makes sense:

A picture may be worth a thousand words - but if you can convey all the information in the text above in two pictures, please let me know and I'll buy you a beer!
IV. Emmetropes
Bonus section! The really interesting thing is that these two events gave a unique insight into two sides of the same world. Here are the main meta-lessons from the two perspectives:
It is impossible to predict the future of healthcare…
Neither group had a firm view on what the future of healthcare looks like
Clinicians would be less frustrated and feel less ignored if they understood how difficult it is for decision-makers to predict future needs and technology, and the inevitable path dependency that occurs.
Decision-makers would be less frustrated if the right clinicians were deeply involved in planning healthcare infrastructure.8 Clinicians will not have all the answers. However, they can help the decision-makers decrease the risk that the physical spaces constrain future development.
… But looking to healthcare’s history can help
Clinical input is key: Clinicians and clinical leaders have been instrumental in shaping how healthcare has developed. Clinicians have transformed healthcare by researching, implementing and evaluating new treatments and processes - which in turn has changed what is needed from our physical buildings. These trends need to be extrapolated in order to understand how healthcare could work in the future.
As one perspective of several: This extrapolation needs a deep understanding from several perspectives: fundamental societal and cultural trends (societies’ needs), medical content (healthcare provision), medical technological development (tools) as well as infrastructural developments (what is possible). Few people can see all perspectives, which is why you need several experts involved. Multidisciplinary analysis is not a buzzword.
The single most important speed-limiting factor is risk appetite
Neither clinicians nor decision-makers have any incentive to bear risk. This is good as we don’t want unsafe treatments or processes, or expensive new buildings which aren’t useful. However, we know that healthcare has transformed throughout history and needs to continue transforming.
If a healthcare system needs to be transformed quicker, then you need to create incentives to bear risk – so that new ideas, processes, modalities and buildings can be tester, iterated and (if successful) scaled.
And finally the most esoteric and unrelated learning of all: ChatGPT 4 refuses to render a hospital room without a window. Despite using numerous prompts during 20 minutes, all hospital rooms had windows. If anyone can explain why that happens, or manages to render a hospital room without a window please let me know! 🪟🤔9
I appreciated several details: 1. Different ratios of clinician to business person in the two worlds. 2. Contrast between abstract knowledge/certificates on one side and physical buildings/things in the other 3. How patients are seen either as miniscule (when planning buildings) or gigantic (when understanding anatomy and pathology) 4. How the image depicts male bias in healthcare management
A rabbit hole I can recommend for Swedish readers is a report by SBU called “The medical development in Sweden during 1960 - 1992”. It’s a treasure trove of snapshots from different specialties - showing how so much has changed, and how quickly we forget what has changed. It was difficult to find, but as an Easter egg to you ardent footnote reader: here it is!
Building a hospital? Read Richard Bohmer’s book Designing Care. He argues that there are two types of care: iterative and sequential. Iterative care occurs when a condition or treatment is unknown, which makes it different to standardize. Sequential care occurs if a condition or management is well understood, and care can be highly reliable and standardized. Bohmer posits that these types of care require different management systems. I would argue that they also require different types of infrastructure.
You probably noted that one outlier, Korea, had a large increase (from 15 to 18.5 days). This seems to be due to growth of “long-term care” hospitals, which function more like nursing homes. I don’t know why they included those hospitals in their statistics.
Some of the countries with the lowest length of stay for heart attacks (e.g. Sweden with 4.1 days in 2019) are also those with the best outcomes. In other words, quality need not correlate to length of stay. Oftentimes higher quality will result in a shorter length of stay.
The source for this is page 62 in the rabbit hole linked in footnote #2. Some rabbit holes are filled with gems. However, when I tried using the term “gem hole”, well, it just didn’t sound right 😅
This is a the kind of phenomenon which is difficult to study as you need to control many confounders and need large cohorts for sufficient power. One article summarizing this has several issues, but I believe it’s probably signal and not just noise and publication bias.
Not necessarily the most senior or experienced clinicians. I believe it’s more important to involved experienced clinicians that are deeply curious, that have a data-based understanding of how their specialty has developed and that have an entrepreneurial mindset. I believe this is needed in order to counteract the status quo bias that always will be prevalent in healthcare (I also believe we need a status quo bias in order to minimize risks for patients due to the intrinsic risk of adopting a new paradigm to easily, but I’ll save that for another post…).
One of Emmetropia’s readers, Nico, had a great question: can’t it simply be that GPT-4 has come to the conclusion that a window is as much part of a hospital room as a bed is? He posed the wise question: can it create a hospital room without a bed? I tried and tried but didn’t succeed despite several prompts. So either (a) the training data has taught the AI that windows and beds are ubiquitous in hospital rooms, or (b) the training data was cleaned to only use rooms with beds and windows to define what a hospital room should look like.